SIROLIMUS-COATED BALLOON: DE NOVO LESIONS · IN-STENT RESTENOSIS · SMALL VESSELS BIFURCATION LESIONS
Clinical Evidence for
MagicTouch SCB
MagicTouch SCB is a polymer-free Sirolimus coated balloon catheter designed for the treatment of coronary artery disease, including de novo lesions, in-stent restenosis (ISR), small vessels, and bifurcation lesions.Engineered with Nanolute Technology, it enables deep vessel wall penetration and sustained drug delivery, supporting optimal vascular healing.
Global evidence
Clinical program
In-Tissue Drug Presence
USFDA IDE APPROVED
ISR · SV
Regulatory Milestone
Clinical Evidence Across Coronary Artery Disease
From real-world registries to investigator-driven global studies, MagicTouch SCB is supported by comprehensive clinical evidence base across de novo lesions, ISR, small vessels & complex ACS populations.
· EASTBOURNE · UK-SEB 2 · SELFIE REGISTRY · FASICO · PICCOLETO VI · NANOLUTE
THE EASTBOURNE Registry – World’s Largest Investigator Driven DCB Prospective Study
ThE All-comers Sirolimus-coaTed BallOon eURopeaN rEgistry
Investigator Driven, Real world prospective global study evaluating the performance of SCB in various coronary lesions to assess the primary endpoint of TLR. 2,123 patients enrolled across multiple centres.
Global Chairman: Prof. Bernardo Cortese
Complex Patient Cohort
Diabetes Mellitus
41.5%
ACS
46.6%
Multi-Vessel Disease (MVD)
59.3%
Previous PCI
66.3%
2-Year Clinical Outcomes
TLR
Minimal Increase in Events at 2 Years
Registry Impact
EASTBOURNE Registry is the world’s largest SCB study in CAD to date, showing promising 1 & 2-year outcomes in real-world patients, with no significant increase in events at 2 years confirming long-term safety of MagicTouch SCB.
*Data published in EuroIntervention Journal: DOI: 10.4244/EIJ-D-23-00966, Volume 20, Number 13 and JACC: Cardiovascular Interventions Vol. 16, No. 14, 2023 – DOI: 10.1016/j.jcin.2023.05.005 | # Planned & Published (# – on sub-studies and publications)
UK-SEB 2 – Assessment of Sirolimus Coated Balloon in Real World Patients
All comers real world patients treated with the MagicTouch Sirolimus Coated Balloon
A prospective, Multicenter, clinical registry that enrolled real world, all comer patients to measure the primary endpoint of Target Vessel Failure at 12 months. 771 patients with de novo coronary lesions in a complex cohort. Median follow-up at 640 days.
Principal Investigator: Dr. Sandeep Basavarajaiah
Diabetes Mellitus
36%
ACS
52%
Small Vessels
78%
Lesions (≥20 mm)
76%
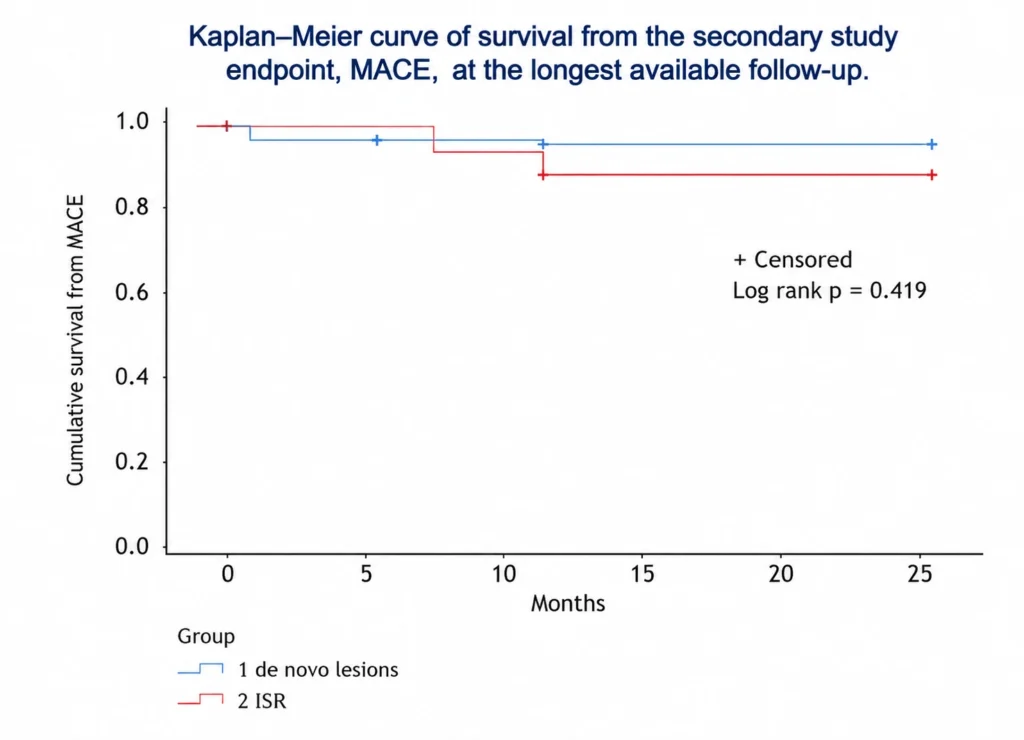
Clinical Outcomes at Median follow-up of 640 Days
MACE at Median
Target Lesion Revascularisation
Target Vessel Myocardial Infarctions
Cardiac Death
Acute Vessel Closure
Target Vessel Revascularisation
Overall Death
Performance in Complex Settings
Diabetes Mellitus vs Non-DM
Small Vessels vs Large Vessels
MagicTouch SCB demonstrated promising results in complex real-world patients with low rates of hard endpoints, acceptable TLR and MACE, and no significant difference across DM vs non-DM and small vs large vessel subsets.
Despite of the complex patient population and lesion subsets, MagicTouch SCB demonstrated promising results
with low rates of hard endpoint (cardiac death and MI), acceptable TLR and MACE. MagicTouch SCB displayed no
significant difference in terms of TLR and TVMI in both DM and Non‑DM group as well as in small vessel versus
larger vessels demonstrating safety and efficacy in actual complex patient subsets
SELFIE Registry
SCB in Acute Coronary Syndrome (ACS)
62 patients evaluated in an investigator-initiated prospective registry assessing the clinical performance of MagicTouch SCB in real-world ACS patients.
Principal Investigator: Dr. Gianluca Caiazzo
Diabetes Mellitus
40%
STEMI
23%
Previous MI
61%
Previous PCI
61%
1-Year Outcomes (11 ± 7 months)
MACE
Target Lesion Revascularisation
Myocardial Infarction & Cardiac Death
Acute Thrombosis & Bleeding
Procedural Outcomes
Procedural Success
Angiographic Success
MagicTouch demonstrated safe and effective outcomes in ACS patients, with high procedural success and low adverse event rates in a complex, real-world setting.
Key Takeaways
The SELFIE Registry is an investigator-initiated prospective study evaluating MagicTouch SCB in 62 real-world ACS patients with high baseline complexity 40% diabetes, 23% STEMI, and 61% with prior MI and prior PCI. At 1-year follow-up (11 ± 7 months), MagicTouch SCB achieved low MACE (4.8%), TLR (3.2%), and MI (3.2%) rates with zero bleeding events. Notably, 100% procedural and angiographic success was achieved across all patients, supporting MagicTouch SCB as a safe and effective treatment option even in high-risk ACS presentations.
1-year outcomes & secondary endpoints of MACEs in de-novo and ISR are similar or lower to previous studies using the same device in different heterogeneous settings or using PCBs in lower-risk population.
Reference: Article published in Journal of Interventional Cardiology By Dr. Gianluca Caiazzo | https://doi.org/10.1155/2020/8865223
PICCOLETO VI
Comparative Functional Outcomes in De Novo CAD
293 unselected patients (227 lesions) evaluated in an investigator-driven, real-world global study comparing multiple drug-coated balloons in de novo coronary lesions.
Principal Investigator: Prof. Bernardo Cortese
Bifurcations (SCB vs PCB)
37.9% vs 31.5%
Ostial Lesions (SCB vs PCB)
22.8% vs 10.8%
DCB size (mm)
2.6±0.5 vs 2.6±0.6
DCB length sum (mm)
31.6±19.1 vs 33.3±18.6
6-Month Angiographic Functional Outcomes
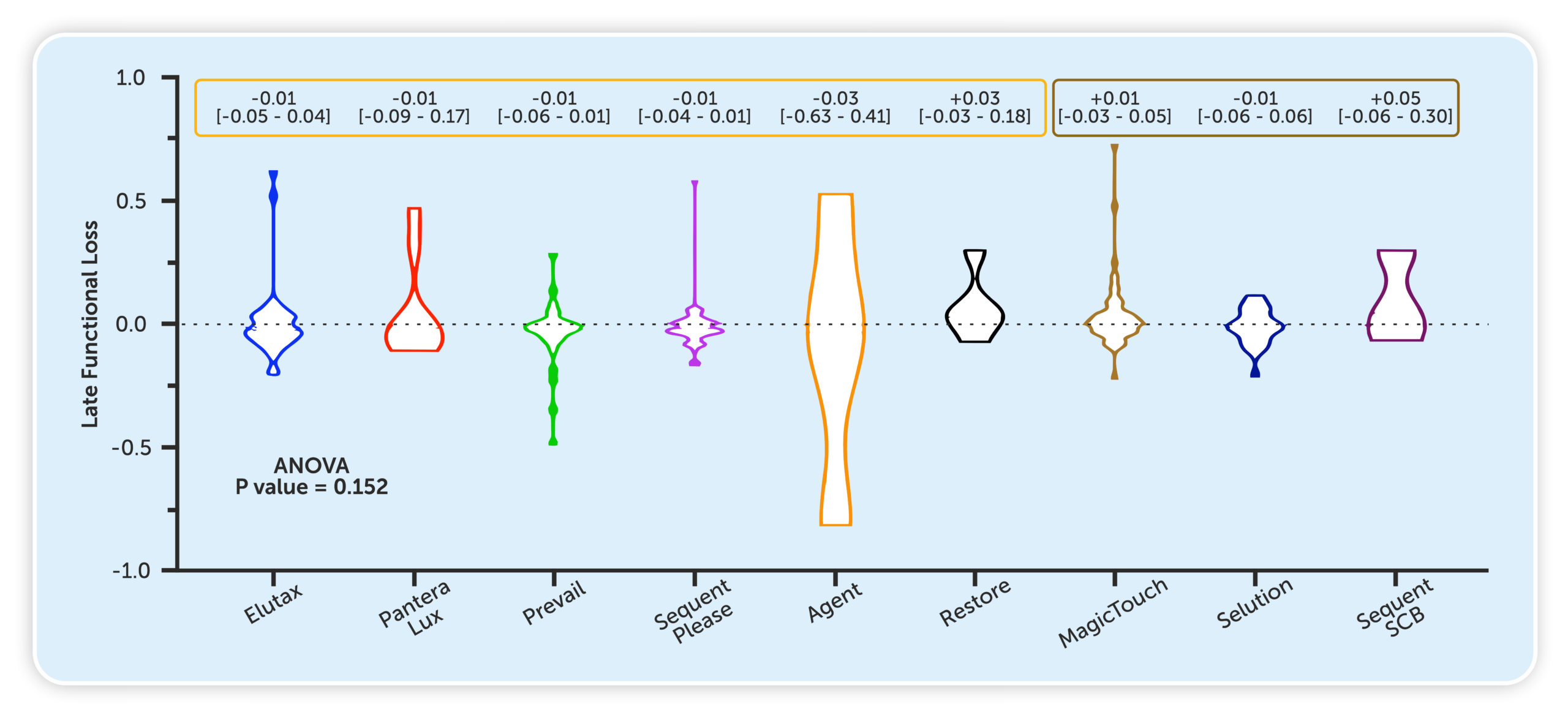
MagicTouch SCB demonstrated comparable functional outcomes in head-to-head evaluation, supporting its use in complex de novo coronary lesions.
Key Takeaways
PICCOLETO VI is the first study directly comparing several types of DCB with angiographic & physiological-derived assessment. The trial studied real world complex settings (44.5% of diffuse lesions) with state-of-the-art lesion preparation. PCB and SCB showed similar late functional loss (core-lab µFR).
Reference: Presented by Prof. Bernardo Cortese at EuroPCR 2025 | Published in AsiaIntervention 2026;12:28-40, DOI: 10.4244/AIJ-D-25-00057
FASICO NATIVES
Angiographic Outcomes in Small Vessel Disease
27 patients evaluated in an investigator-driven prospective registry assessing the angiographic performance of MagicTouch SCB in native coronary vessels (<3mm).
Principal Investigator: Prof. Bernardo Cortese
Key Angiographic Endpoints at 6 – Months
Minimal Lumen Diameter (MLD)
MagicTouch SCB demonstrated strong angiographic performance with minimal late lumen loss, maintaining good vessel patency at follow-up in native vessel coronary disease.
Key Takeaways
FASICO NATIVES is an investigator-driven prospective registry evaluating MagicTouch SCB in 27 patients with native small vessel coronary disease (<3mm). At 6-month angiographic follow-up, exceptionally low late lumen loss (0.09 ± 0.34 mm) was observed, with strong lumen gain of 0.82 ± 0.38 mm from baseline. MLD was well maintained from post-procedure (1.68 ± 0.48 mm) to follow-up (1.59 ± 0.59 mm), FASICO Natives revealed promising & positive angiographic data of a Sirolimus Coated Balloon treatment at 6-months. The study confirms the effectiveness of MagicTouch SCB for the treatment of de novo coronary
lesions by maintaining good vessel patency at angiographic follow-up with interesting signs in terms of LLG.
Reference: Article published in Journal of Cardiovascular Medicine 20(7):p 471-476, July 2019. I DOI: 10.2459/JCM.0000000000000806
NANOLUTE
Long-Term Evaluation in Real-World Population
450 patients evaluated in a prospective, multicenter study assessing the safety and efficacy of Sirolimus Coated Balloon in real-world coronary artery disease.
Principal Investigator: Dr. Sameer Dani
Diabetes Mellitus
45.3%
De Novo Lesions
53%
ISR
47%
ACS
48.2%
3-Year Long-Term Clinical Outcomes
6-Month Key Endpoints
Demonstrates Sustained Safety – Up to 3 Years
No significant increase in adverse events across 1, 2 and 3-year follow-up timepoints
1-Year Outcomes
2-Year Outcomes
3-Year Outcomes
NANOLUTE study demonstrates low rates of adverse clinical events with sustained outcomes up to 3 years, supporting the safety and effectiveness of MagicTouch SCB in real-world coronary artery disease.
Key Takeaways
NANOLUTE is a prospective, multicenter study evaluating MagicTouch SCB in 450 real-world patients with coronary artery disease, including a high proportion of ACS (48.2%), de novo lesions (53%), ISR (47%), and diabetes (45.3%). Procedural success was near-perfect at 99.6%. Early MACE was low at 3.3% at 6 months. Long-term follow-up showed stable outcomes across 1, 2, and 3 years, with MACE reaching 6.7% and TLR/TVR 4.7% at 3 years — consistent with the expected natural history of complex CAD. These results confirm the durable safety and efficacy of MagicTouch SCB as a real-world all-comer treatment strategy.
Reference: https://doi.org/10.1016/j.jacc.2022.03.063
Sirolimus Coated Balloon Catheter
Effective treatment solution for de novo lesions, ISR, small vessel disease, and bifurcation lesions.
- Circumferential coating for uniform drug distribution during inflation
- Optimized re-wrap to minimize in-transit drug loss
- Polymer-free design to support vascular healing
- Nanolute® Technology for enhanced vessel wall penetration
- 2 US FDA IDE Approval for Small Vessels & In-Stent Restenosis Indications
Encapsulation of sub-micron Sirolimus in phospholipid carriers enables deeper vessel wall penetration and efficient drug delivery.
Sirolimus availability within the vessel wall is maintained for up to 120 days, aligning with the natural vascular healing window.
MagicTouch SCB at a Glance
A next-generation SCB platform combining precision drug delivery, clinical validation, and real-world performance
MagicTouch SCB is a Sirolimus-coated, polymer-free balloon catheter designed for coronary interventions, enabling uniform drug distribution and sustained therapeutic effect.
Backed by the most comprehensive clinical trial program for sirolimus-coated balloons in coronary interventions, including 19 trials and ~9,000 patients.
Target Lesion Subsets
Indicated for treatment of:
- De novo coronary lesions
- In-stent restenosis (ISR)
- Small vessel disease
- Bifurcation lesions
Why Sirolimus for Coronary Interventions?
Sirolimus delivers anti-proliferative and anti-inflammatory effects with a broad therapeutic window, supporting controlled vascular healing.

From balloon to vessel wall
Nanolute Technology synchronizes drug delivery and retention with the vessel healing timeline, enabling effective therapy at the target site.
Nanolute® Technology &
Device Engineering
MagicTouch SCB integrates advanced Sirolimus delivery technology with an optimized balloon platform to balance deliverability and sustained drug transfer.

Built for Coronary Complexity
A low crossing profile with enhanced flexibility supports access to complex coronary anatomies, including small vessels and bifurcations.
- Optimized crossing profile
- High flexibility
- Stable coating integrity
- Wide lesion coverage
Clinical resources &
next steps
Access detailed study data, product documentation, and support resources.
Access product details
The law restricts this device to sale by or on the order of a physician. Refer to the Instructions for Use (IFU) for full indications, contraindications, warnings and precautions.
For use only in countries where MagicTouch SCB is registered with applicable health authorities. Approved by USFDA use in clinical trials only.